Ligament Sprain or Repair
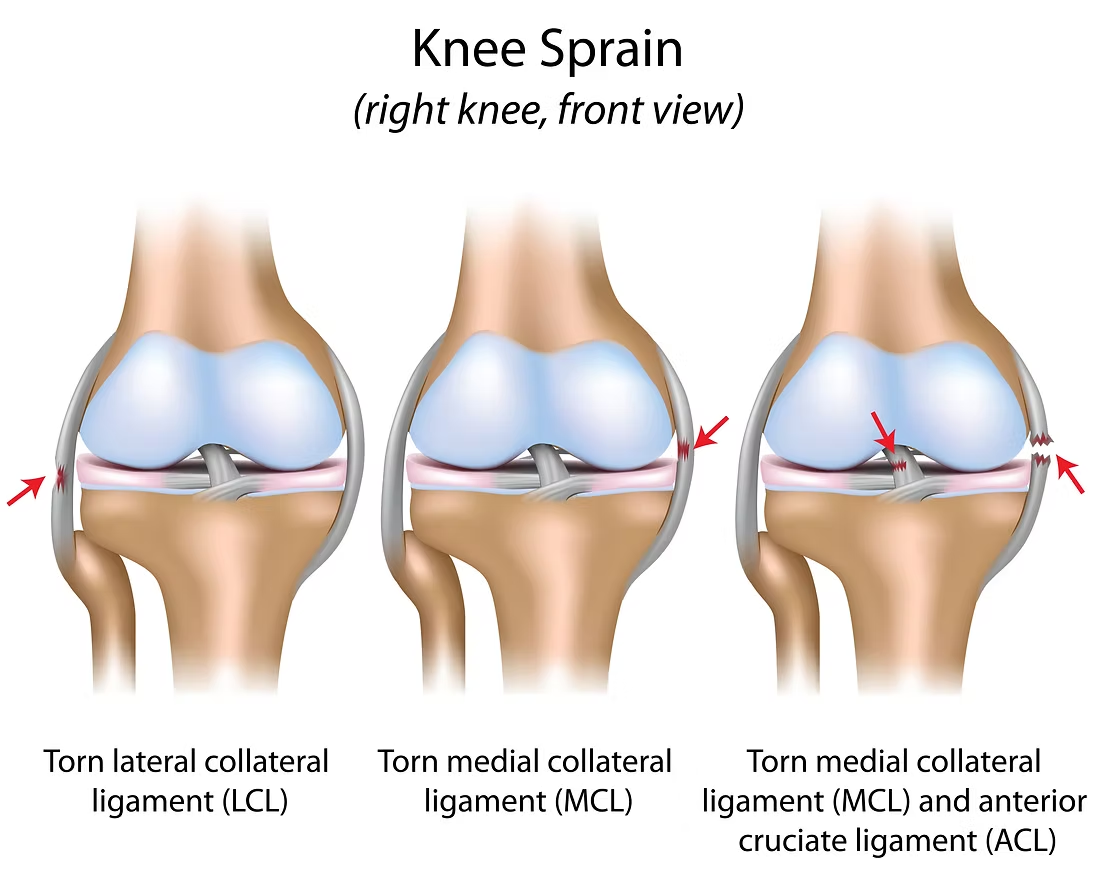
There are 4 major ligaments of the knee. These are the ACL, the MCL, the LCL, and the PCL.
.svg)
.svg)
There are 4 major ligaments of the knee. These are the ACL, the MCL, the LCL, and the PCL. These ligaments are responsible for maintaining stability in our knee joint when we walk, run, and complete any weight bearing activity. Any one of these ligaments can be sprained or torn based on the patient case. A grade 1 sprain is diagnosed as a slight stretch of the ligament but it remains in tact. A grade 2 sprain is a partial tear of the ligament. A grade 3 sprain is a full tear of the ligament. Each of these ligaments will be discussed below.
The ACL (the Anterior Cruciate Ligament) runs from the femur to the tibia diagonally across the front of the knee joint. It helps provide front to back stability of the knee and prevents the tibia (the lower bone of the knee) from moving too far forward when we walk or run. ACL sprains or tears are especially common in athletes, those participating in higher level movements, or those involved in traumatic accidents. ACL injuries often times occur as a result of a non contact injury when there is a muscle imbalance between the quadricep and the hamstring. When an individual accelerates and decelerates quickly the quadricep can contract forcefully without an equal contraction from the hamstring leading to an ACL sprain/tear. The extent of the ACL sprain and its management is entirely dependent upon the individual and the case. Patients who suffer an ACL sprain will almost always be sent to physical therapy before any surgical intervention is considered. There are a couple reasons for this. The first being surgery may not be necessary! Most people who suffer an ACL injury immediately think they will need surgery and have to go through a lengthy rehabilitation but this is not true. The management of ACL injuries has changed dramatically in recent years. We now know we can distinguish people into two categories; copers and non-copers. Copers are individuals with ACL tears who can cope with the ACL tear. Meaning they function and live a normal life without their ACL in tact. Copers can do this because they have adequate quadricep strength that provides their knee enough stability that they do not actually need their ACL to be in tact. A great example of this I give patients is a retired football named Hines Ward. Hines Ward was professional NFL player who found out he had a full ACL tear by accident during a physical when he was preparing for the draft. It turns out he tore the ACL in elementary school in a bike accident. He played his entire high school and college career with a torn ACL and had no clue! He opted to not have surgery and ended up playing over 10 years in the NFL winning super bowl MVP and being named to numerous all pro teams, all without having a left ACL. The example with Hines Ward is also true for many. There are potentially upwards of tens of thousands of people across the globe who have torn ACL's and have no idea because they cope so well. In physical therapy we work to build sufficient quadriceps strength to prevent feelings of buckling or instability from the torn ACL. If this is successful then a patient may not need surgery. Sometime despite strengthening the patient will still have feelings of buckling or instability in the knee. These individuals are referred to as noncopers and often referred for an ACL reconstruction surgery. Physical therapy is still important prior to surgery because the prognosis after surgery is better if the patient has greater mobility and strength.
ACL reconstruction surgery is a minimally invasive arthroscopic procedure that takes a tissue graft from either the hamstring tendon, the quadricep tendon, the patella tendon, or a tissue donor and uses this graft to make the new ACL. After surgery patients may have lingering pain in the knee, and will have limited range of motion and strength. In physical therapy we work to address all of these concerns. Our goal is to minimize pain and restore range of motion and strength levels to what they were before the injury using either a surgeon dependent protocol or a general protocol. Patients who undergo ACL reconstruction tend to have excellent results and return to their normal activities without limitations.
The MCL, or Medial Collateral Ligament, runs from the femur to the tibia on the inside of the knee and resists side to side motions at the knee. Most often the MCL is injured by a direct force to the outside of the knee. This causes the knee to collapse in and stress the MCL causing sprain or rupture. The MCL generally has good blood flow which allows it to heal on its own. The healing timeframe depends on the extent of the sprain. If the MCL is fully torn it may require a surgical repair depending on the surgeon diagnosis. MCL injuries requiring surgical repair are considered to be severe and often involve other structures within the knee such as the ACL and meniscus (when these 3 are injured together it is referred to as an unhappy triad). In this case the MCL will be repaired with a graft. Following an MCL sprain we work to reduce any pain that may be present, we work to restore any losses of motion, and we work to improve strength levels around the knee to what they were prior to the injury.
The LCL, or Lateral Collateral Ligament runs from the femur to the tibia on the outside of the knee and resists side to side motions at the knee. The LCL is often injured by a direct force to inside of the knee. This causes the knee to move outwards and stress the LCL to sprain or rupture. The LCL generally has good blood flow which allows it to heal on its own. The healing timeframe depends on the extent of the sprain. If the LCL is fully torn it may require a surgical repair depending on the surgeon diagnosis. LCL injuries requiring surgical repair are considered to be severe and are often repaired because the injuries involves other structures within the knee such as the ACL or meniscus. In this case the LCL will be repaired with a graft. Following an LCL sprain we work to reduce any pain that may be present, we work to restore any losses of motion, and we work to improve strength levels around the knee to what they were prior to the injury.
The PCL, or Posterior Cruciate Ligament, runs from the femur to the tibia in a diagonal fashion across the back of the knee. The PCL is responsible for resisting front and back motions at the knee. PCL injuries are commonly referred to as “dashboard injuries” because most cases involve a direct below to the lower leg below the knee. Injuries to the PCL alone are rare and much less prevalent than injuries to the ACL. When the PCL is injured other ligaments or internal damage within the knee is almost always present. Surgery is not always indicated following a PCL sprain but severe cases may require a PCL reconstruction in which the surgeon will arthroscopically reattach the PCL using a graft. Following a PCL sprain we work to reduce any pain that may be present, we work to restore any losses of motion, and we work to improve strength levels around the knee to what they were prior to the injury.
For examples of how we treat ligament injuries in our clinic please see the photos below. If you would like to schedule an appointment please reach out to us.










Whether you're recovering from an injury, managing chronic pain, or looking to improve mobility, our team at Andrew's Physical Therapy is here to guide you.
Contact Us Posture related pain is often referred to as “Upper Crossed Syndrome”. It is extremely common and we are seeing more and more of it in physical therapy.
Shoulder impingement is one of the more common causes of shoulder pain. Shoulder impingement occurs when the supraspinatus
ennis Elbow, medically referred to as lateral epicondylitis, is an overuse injury that effects two muscles in the outer elbow called the extensor